Phillip Buckhaults, a cancer genomics expert, and professor at the University of South Carolina has testified before a South Carolina Senate Medical Affairs Ad-Hoc Committee saying that Pfizer’s mRNA vaccine is contaminated with billions of tiny DNA fragments.
Buckhaults, who has a PhD in biochemistry and molecular biology, said “there is a very real hazard” that these fragments of foreign DNA can insert themselves into a person’s own genome and become a “permanent fixture of the cell.”
He said it’s a plausible mechanism for what might be “causing some of the rare but serious side effects like death from cardiac arrest” in people following mRNA vaccination.
Buckhaults is not an alarmist and has been reluctant to go public with his findings for fear of frightening people.
He himself was vaccinated three times with Pfizer’s covid vaccine and recommended it to family and friends. He described the mRNA platform technology as “revolutionary” and said the vaccine has saved many lives.
“I’m a real fan of this platform,” Buckhaults told the Senate. “I think it has the potential to treat cancers, I really believe that this platform is revolutionary. In your lifetime, there will be mRNA vaccines against antigens in your unique cancer. But they’ve got to get this problem fixed.”
Buckhaults is most concerned about the “very real theoretical risk of future cancer in some people, depending on where this foreign piece of DNA lands in the genome, it can interrupt a tumour suppressor gene or activate an oncogene.”
“I’m kind of alarmed about this DNA being in the vaccine… DNA is a long-lived information storage device. It’s what you were born with, you’re going to die with and pass on to your kids. … So alterations to the DNA…well, they stick around,” he said.
Buckhaults believes the vaccines were deployed in good faith, but given the panic and urgency of the crisis, “there were a lot of shortcuts taken.” He puts it down to incompetence not malice, quoting Hanlon’s razor…
“…. which is never attribute malice to that which can be better explained by incompetence. There could be malice underneath, but I’m trying to see just incompetence to be gracious,” he told the Senate.
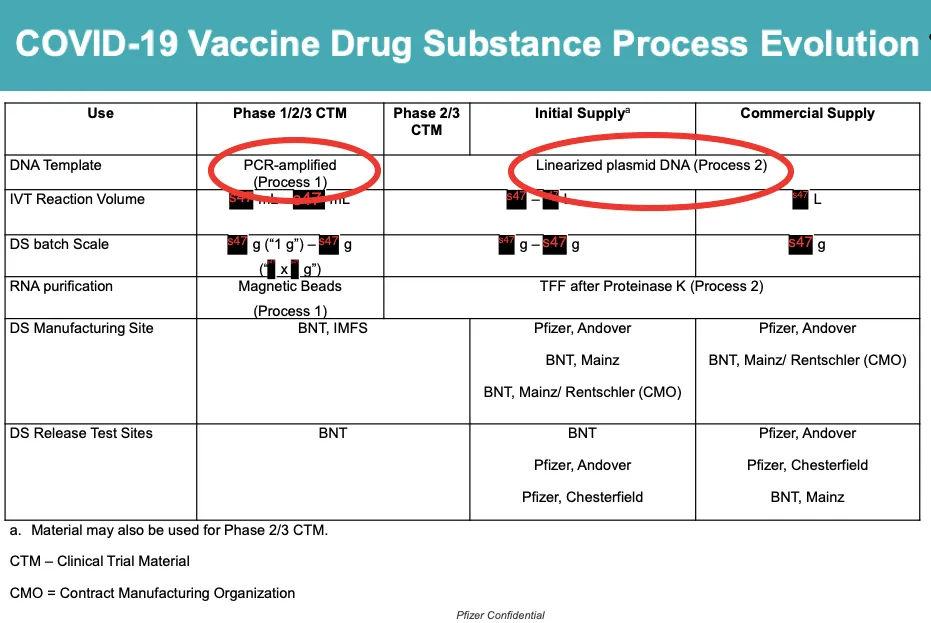
Buckhaults explained how two different manufacturing processes were used to make Pfizer’s vaccine.
The initial production of Pfizer’s covid vaccine used a method called Polymerase Chain Reaction (PCR) to amplify the DNA template that was then used for production of the mRNA. This method, called PROCESS 1, can be used to make a highly pure mRNA product.
However, in order to upscale the process for large-scale distribution of the vaccine to the population for its “emergency authorisation” supply, Pfizer switched to a different method – PROCESS 2 – to amplify the mRNA.
PROCESS 2 used bacteria to make large quantities of “DNA plasmid” (circular DNA instructions), which would be used to make the mRNA. Hence, the final product contained both plasmid DNA and mRNA.
The switch from PROCESS 1 to PROCESS 2, ultimately resulted in the contamination of the vaccine (see red circles).
Pfizer tried to deal with the problem by adding an enzyme (DNAse) to chop up the plasmid into millions of tiny fragments.
But Buckhaults said it made the situation worse because the more fragments you have, the greater the chance that one of the fragments inserts itself into the genome and disrupts a vital gene.
“[Pfizer] chopped them up to try to make them go away, but they actually increased the hazard of genome modification in the process,” explained Buckhaults.
“I don’t think there was anything nefarious here, I just think it was kind of a dumb oversight,” he added. “They just didn’t think about the hazard of genome modification…it’s not all that expensive to add another process to get it out.”
A BMJ investigation found that batches of vaccine derived from PROCESS 2, were shown to have substantially lower mRNA integrity, and some say these vaccines have been associated with greater adverse events.
Buckhault’s research is not an outlier. Genomics expert Kevin McKernan has also reported plasmid DNA contamination in both Pfizer and Moderna bivalent covid-19 vaccines, in amounts that far exceeded the safety limit set by the FDA.
The FDA acknowledges that there are risks to having residual DNA left in vaccines:
Residual DNA might be a risk to your final product because of oncogenic and/or infectivity potential. There are several potential mechanisms by which residual DNA could be oncogenic, including the integration and expression of encoded oncogenes or insertional mutagenesis following DNA integration. Residual DNA also might be capable of transmitting viral infections if retroviral proviruses, integrated copies of DNA viruses, or extrachromosomal genomes are present.
In its guidance to industry, the FDA says:
The risks of oncogenicity and infectivity of your cell-substrate DNA can be lessened by decreasing its biological activity. This can be accomplished by decreasing the amount of residual DNA and reducing the size of the DNA (e.g., by DNAse treatment or other methods) to below the size of a functional gene (based on current evidence, approximately 200 base pairs). Chemical inactivation can decrease both the size and biological activity of DNA.
The problem with this advice said Buckhaults, is that it applies to the manufacturing of traditional vaccines, which contain what is known as “naked DNA.”
Normally, low levels of naked DNA in a vaccine would not be a problem because the bits of DNA are chewed up by tissue enzymes before they’ve had a chance to get inside cells. However, the DNA in Pfizer’s vaccine is not “naked.”
It is wrapped up in lipid nanoparticles (LNPs) – essentially fat globules – that help transport the genetic material (mRNA and plasmid DNA) inside the cells where the DNA can migrate to the nucleus and insert itself into the genome.
That’s why Buckhaults told the Senate that the FDA’s rules for safe levels of DNA in vaccines does not apply to the new mRNA platform technology.
“The fact that there is a regulatory threshold for the amount of DNA allowed in a vaccine is a throwback to an era when we were talking about [traditional] vaccines…but they inappropriately applied that regulatory limit to this new kind of vaccine where everything is encapsulated in this lipid nanoparticle — this was an inappropriate application of an old school regulation to a new kind of vaccine,” said Buckhaults.
Buckhaults said that vaccinated people need to be tested to see if any of the foreign DNA has integrated into the genome of their stem cells. This is easily detectable because the foreign DNA has a unique signature. Buckhaults said “It leaves a calling card.”
“This is not terribly expensive to do these kinds of tests,” he added, “But there has to be a system where professors are not going to be penalised for producing results that are counter to what the party line is supposed to be.”
Senator Billy Garrett asked whether Buckhaults could test for DNA contamination in the new covid boosters that the Biden administration just recommended for all Americans aged 6 months or older.
“I would like to do that,” said Buckhaults. “It takes about three hours to check a vial of vaccine to see if it’s got this in it – about 100 bucks of reagents.”
“And I will not get the vaccine again myself unless I get a batch and find out that it’s free of DNA,” he added.
While the Senators offered to intervene if Buckhaults received any retribution or harassment in response to his testimony at the hearing, they did appear helpless in their ability to bring about meaningful change.
Senator Richard Cash said, “We are not going to have any authority over the FDA to force Pfizer to do something. I mean, that’s a federal issue.”
Buckhaults told the Senate that he emailed the FDA about the contamination problem but had not received a reply.
The FDA has been approached for comment.