In reporting on a Montana case in which a judge ruled that the state had to include the climate effect of oil and gas permits before deciding on them, the Associated Press showed just how brain-dead the discussions of “global warming” have become.
District Court Judge Kathy Seeley ruled in favor of several young plaintiffs – ranging in age from 5 to 22 – saying they “have a fundamental constitutional right to a clean and healthful environment, which includes climate as part of the environmental-support system.”
As proof of the harm the plaintiffs are suffering, the order has a list of horribles that includes:
“Olivia expressed despair due to climate change.”
“Badge is anxious when he thinks about the future that he, and his potential children, will inherit.”
“Grace … is anxious about climate change.”
“Mica gets frustrated when he is required to stay indoors during the summer because of wildfire smoke.”
(Perhaps the judge should have ruled against the adults who are filling these poor children’s minds with climate alarmist fantasies, but that’s another story.)
The ruling was heralded by the likes of Julia Olson, executive director of the Oregon-based Our Children’s Trust, which has filed similar lawsuits in other states, who said: “Today’s ruling in Montana is a game-changer that marks a turning point in this generation’s efforts to save the planet from the devastating effects of human-caused climate chaos.”
(Apparently, after “global warming,” and “climate change,” and “climate crisis” failed to move the needle, the left is trying out “climate chaos.”)
We will admit that we find ourselves in wholehearted agreement with Emily Flower, spokesperson for Montana Attorney General Austin Knudsen, who called the ruling “absurd” and said that this “same legal theory has been thrown out of federal court and courts in more than a dozen states. It should have been here as well, but they found an ideological judge who bent over backward to allow the case to move forward and earn herself a spot in their next documentary.”
In any event, it was up to the crack reporters and editors at the once respectable Associated Press to come up with what is perhaps the most asinine sentence ever written about this issue.
“The ruling following a first-of-its-kind trial in the U.S.,” the AP reported, “adds to a small number of legal decisions around the world that have established a government duty to protect citizens from climate change.”
“A government duty to protect citizens from climate change”?
Think about that for a minute.
Do they mean any sort of climate change, such as the climate change that occurs around the world every year when temperatures can change from sub-zero to 90 degrees in a matter of months?
Or perhaps they mean that the government should protect citizens from things like El Nino, that naturally recurring – but scientifically inexplicable – climate phenomenon that we are currently experiencing, and underwater volcanic eruptions, both of which have driven this summer’s heat waves.
Or, longer term, what about ice ages? There have been five of them in the earth’s history – also for reasons nobody can fully explain. The last one ended 10,000 years ago, which is about how long these “interglacial” periods last. A few years ago, some researchers predicted the next ice age could begin in 2030. Is it the government’s duty to protect us from this climate variation?
Someone should take these AP reporters aside and explain to them a basic fact of life: The climate is always changing. Always. Sometimes for the worse. Sometimes for the better.
They might go on to explain to these reporters that the best way to deal with an ever-changing climate isn’t to wish change away, or pretend that denying a drilling permit will make one iota of difference, but to encourage human ingenuity and prosperity.
That’s how you deal with a climate that is always changing. By adapting to it. It’s why deaths from naturally occurring disasters such as earthquakes, hurricanes, and so on, have steadily fallen as mankind has become smarter and more prosperous.
It’s radical anti-growth environmentalists – aided by brain-dead reporters – not oil and gas companies, who are the biggest threats to the health, safety, and well-being of those kids in Montana.
Just putting this out there. Fauci successor at NIAID peddled dangerous Remdesivir drug as ‘silver bullet’ against Covid-19 Dr. Jeanne Marrazzo tried to use unsafe antiviral IV drug on every covid hospitalized patient at UAB.
Dr. Jeanne Marrazzo, the newly minted successor to Dr Anthony Fauci at the National Institute for Allergy and Infectious Diseases (NIAID), was recently one of America’s chief hype women for an antiviral drug that is now unanimously considered an unsafe and catastrophically failed treatment for Covid-19.
Prior to moving to her Government Health post, Marrazzo was the longtime director of the Division of Infectious Diseases at the University of Alabama at Birmingham (UAB).
In partnership with Big Pharma drugmaker Gilead, UAB played a major role in the research and development of Remdesivir. The drug was developed over a decade ago with the hopes to treat Hepatitis C and respiratory syncytial virus (RSV), but was suddenly repurposed to “treat” Covid-19 when coronavirus hysteria reached the United States.
Given the UAB-Gilead partnership, one would think that Dr. Marrazzo would refrain from commenting on issues through which she maintained a clear conflict of interest. Or at the very least, she had the duty to disclose her conflict of interest when speaking to the media about the UAB-developed “wonder drug.” She did no such thing.
Even worse, Dr. Marrazzo bashed harmless and low cost alternatives like hydroxychloroquine, while hyping the super expensive Gilead-UAB competitor drug.
“The hope was maybe, if you treat early in the disease, you don’t need a silver bullet” such as remdesivir, she told The Washington Post in a July 2020 piece. “Hospitals are on the razor’s edge,” she added, contributing to the fear and paranoia that was enveloping the nation at the time.
In interview after interview, Dr. Marrazzo had nothing but good things to say about remdesivir, despite the incredible lack of data available to support her outandish claims about the drug.
On social media, Marrazzo lavished endless praise upon Remdesivir, declaring it the best agent against coronavirus disease, and boasting that her hospital tries to use it on every covid-hospitalized patient.
“We don’t have enough remdesivir to treat everybody who’s in the hospital,” she said in a late 2020 news conference about the state of her hospital system. “It’s a really challenging situation.”
Her predecessor at the NIAID, Mr Fauci, infamously paraded Remdesivir as the “standard of care” for Covid-19 treatment, adding that it can “block the virus.”
Unsupported pseudoscientific claims about very expensive drugs (a full course of remdesivir costs the patient thousands of dollars) is nothing new for NIAID officials, who, under Fauci’s leadership, have created an agency that acts as a government marketing department for pharmaceutical companies.
Undoubtedly, Marrazzo’s Remdesivir maximalism had disastrous implications for patients hospitalized at UAB. The so-called silver bullet later took on a morbid nickname, “run, death is near,” because of the severe side effect portfolio associated with the IV drug.
The headlines speak for themselves:
Remdesivir not only failed, but actively harmed hospitalized patients, who were being injected with the antiviral agent following the recommendations of Dr. Marrazzo.
The most exhaustive studies on the Gilead-UAB drug show that there are zero clinical benefits to injecting patients with remdesivir. Many studies show that Remdesivir can severely injure vital organs such as the heart and kidneys.
Dr. Marrazzo has never publicly expressed remorse for her longtime promotion of the drug she once described as a “silver bullet” against Covid-19. She last promoted the unsafe drug in December, 2021, long after most hospital systems stopped treating patients with the Gilead-UAB disaster drug.
Last week during an Australian Senate committee hearing, Pfizer and Moderna executives were grilled under oath about covid-19 vaccine policies and vaccine safety.
Tensions were high during the public hearing, which was live-streamed via the parliamentary website.
Senators fired questions at Pfizer and Moderna executives who responded by dodging questions and refusing to take accountability for their failures.
To complicate matters, the drug company executives did not attend the hearing in-person, only via video link allowing them to plead ignorance about the studies that were presented during the inquiry.
At the commencement, the Chair warned the witnesses against giving “false or misleading evidence” and after opening statements by Pfizer and Moderna, the floor was opened to questions.
Stopping transmission
Senator Matt Canavan began question time and was laser-focused on the issue of viral transmission.
“Did Pfizer test whether your covid-19 vaccine could stop or reduce the transmission of the virus before its approval and rollout in late 2020,” asked Canavan pointedly.
Pfizer Australia’s medical director Krishan Thiru was evasive.
Left to right: Brian Hewitt, Director of Regulatory Affairs, Pfizer Australia; Krishan Thiru, Medical Director, Pfizer Australia
“To bring this vaccine to patients we were required to show that the vaccine was safe and effective…The primary purpose of vaccination was, and remains, to protect the person who received the vaccine,” said Thiru.
Canavan reminded him that Pfizer’s own CEO Anthony Bourla told a reporter on NBC news on Dec 3, 2020, that it was “not certain” if vaccinated people could catch and spread the virus, but Thiru kept repeating the mantra, “the vaccine is safe and effective.”
Canavan persisted, citing Pfizer’s official tweet on Jan 14, 2023, stating its highest priority was its “ability to vaccinate at speed to gain herd immunity and stop transmission,” and then on June 8, 2021, Bourla tweeted, “the vaccine was a critical tool to help stop transmission.”
“What evidence did Pfizer have to make that public statement to imply that vaccination could stop transmission?” asked Canavan.
Thiru pleaded ignorance saying he was not familiar with the context of the tweets and took the question on notice (to respond later in writing).
Canavan explained that federal and state governments had imposed vaccine mandates based on the evidence and advice from the manufacturers that claimed the vaccines could “stop the spread.”
Canavan also pointed to the Doherty Modelling report submitted to national cabinet in Nov 2021 that underpinned the government’s decision to impose mandates in late 2021, but again, Pfizer could not confirm whether it was consulted about the modelling.
Hewitt said, “I can’t answer that question” and took it on notice.
Moderna Executive Director of Medical Affairs for Respiratory Vaccines Rachel Dawson, said that in the phase III pivotal trials of 2020, its mRNA vaccine showed that it could reduce symptomatic infection, and that it could “make an important contribution to reducing viral transmission.”
Dawson cited real world data demonstrating that the spread of the virus was reduced in households among vaccinated individuals and that they had a “lower viral load.”
But to this day, the US regulator says the ability of Moderna’s mRNA vaccine to reduce transmission remains unproven. “While it is hoped this will be the case, the scientific community does not yet know if Spikevax will reduce such transmission,” states the FDA.
Canavan said Moderna’s evidence, “just doesn’t seem to stack up”.
“Politicians told us it will stop the spread. Clearly that hasn’t happened. Do you have a simple explanation for why very high rates of vaccination, higher than anyone expected (90%) in this country, has clearly not stopped the spread of coronavirus,” asked Canavan.
But Moderna avoided the question on transmission, presumably because it would undermine the entire argument that vaccine mandates “keep others safe,” and instead, referred to its scripted statement that “the goal of vaccination is to prevent severe infection in hospitals.”
Preventing infection
Senator Gerard Rennick then proceeded to challenge Pfizer on its claim that the vaccine was “100% effective at preventing covid-19 cases,” a statement that Bourla tweeted on April 2, 2021.
Rennick proceeded to explain why the statement was implausible.
“By September 2022, Australia had recorded 10 million cases of COVID despite having an adult population vaccinated to the tune of 95% so given those real world figures in Australia, do you still stand by that statement?” said Rennick.
But Thiru responded repeatedly, “we strongly believe, and we reiterate, that the vaccine is safe and effective for its intended use” saying that Pfizer’s vaccine remained highly effective prior to the emergence of variants.
When Rennick asked Pfizer for its definition of “highly effective” in terms of duration, Thiru responded saying, “When the wild-type virus was prevalent, efficacy of approximately or greater than 90% was maintained at six months for illness and severe disease.”
But regulatory filings clearly show Pfizer had strong evidence by April 2021 that its vaccine’s efficacy waned, and withheld the data from the public for months.
Claiming that vaccine efficacy was 90% after six months following vaccination is misleading because that figure is largely driven by the first couple months of the trial when there was still a placebo group. Had people stayed in the trial for the whole duration of the 6 months, the average overall, would have been lower.
Lack of studies
Senator Rennick proceeded to read out the TGA’s non-clinical report listing all the safety studies in animals that were not carried out prior to testing in humans.
Despite assurances that “no corners were cut,” there were no carcinogenic tests, genotoxicity tests, immunotoxicity tests, duration studies, interaction studies with other medicines, and the list went on.
Again, Thiru predictably answered, “I don’t have that report in front of me, so I’m afraid I can’t talk to that.”
When Rennick asked directly if any studies were omitted or circumvented entirely to achieve the accelerated time frame for vaccine development, Pfizer objected saying its process was “thorough and comprehensive”.
Safety problems
Senator Rennick asked if Pfizer had determined the mechanism for why its vaccine could cause myocarditis and pericarditis, but Thiru was defiant saying that Pfizer had “strong confidence in the safety profile” of its vaccine.
Rennick would not let up. “I want you to explain to me why it causes myocarditis,’ he asked several times.
Thiru conceded that Pfizer was aware of “very rare” reports of myocarditis and pericarditis temporally associated with vaccination, but could not explain the mechanism, instead opting to take the question on notice again.
Senator Alex Antic challenged Pfizer on the Fraiman re-analysis, which found one additional SAE for every 800 people vaccinated with an mRNA vaccine, but his attempts hit a brick wall.
Senator Pauline Hansen chimed in, noting the Fraiman re-analysis found a “36% increase in serious adverse events. The most common were coagulation disorders, including thrombosis, and acute cardiac injury. In every 10,000 people injected 18 will experience a life threatening or altering medical complication,” said Hansen.
Again, Thiru pleaded ignorance. “I do not have a copy of your paper. I have not examined it,” he said, “the benefit risk ratio for vaccination remains strongly positive in all indications, all age groups for which it has been approved.”
Senator Hansen became visually frustrated.
“You haven’t read up on all of this, have you?” she said angrily, “You’ve come to this inquiry and you haven’t done anything whatsoever to respond to our questions. I think it’s very poor of you to not be able to answer these questions.”
When it was Moderna’s turn to respond to the Fraiman re-analysis, they too, said they were not aware of it.
Senator Antic asked Moderna what its overall rate of SAEs was for its mRNA vaccine and how that compared to routine vaccination.
But Moderna’s director of Scientific Leadership Chris Clarke said, “I don’t have the actual rates of adverse events,” as he shuffled through the papers on his desk.
Antic was staggered by the response, “You’re before a Senate inquiry and you cannot tell me the rates of serious adverse events? I mean, it’s quite extraordinary.”
Moderna took the question on notice and said that in the clinical trials they “observed no safety concerns.”
Indemnity agreements
Senator Malcolm Roberts asked for details of the indemnity agreement between Pfizer and the Australian government.
Specifically, Roberts asked if there was any clause in the agreement that indemnified Pfizer in the situation where an employee is mandated by their employer to undergo vaccination and then experiences harm.
“Senator, any indemnity agreements between Pfizer and the Australian Government are confidential, and we’re not able to discuss that in this forum,” responded Thiru.
Roberts fired back, “What have you got to hide?”
He also asked if there was any clause in the agreement that negates Pfizer’s indemnity in the event Pfizer is found to have committed fraud in the trial, as alleged by whistle-blower Brook Jackson in 2021.
“My question is simple. What is the answer? Yes or no?” asked Roberts. But Pfizer insisted “the contents of Pfizer’s contract with the Australian Government remains confidential.”
Senator Malcolm Roberts summed up his thoughts.
“You have repeatedly refused to provide evidence and dodged questions from Senators Rennick and Antic. You have relied instead on appeals to authority, and other logical fallacies.”
Covid vaccine in pregnancy
Senator Hansen confronted Pfizer with questions about the safety of its vaccine in pregnant and breastfeeding women.
Thiru did concede that there is limited clinical trial evidence in pregnant women, but said that peak bodies such as the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) supported use of the vaccine.
“[RANZCOG] have said pregnant women in Australia are a priority group for covid-19 vaccination and should be routinely offered the Pfizer vaccine (Comirnaty) or Moderna (Spikevax) vaccines at any stage of pregnancy. They have said there is no evidence of increased risk of miscarriage or teratogenic risk with mRNA or viral vaccines.”
Forced vaccination
One of the most egregious moments of the hearing was when Pfizer’s Head of Regulatory Affairs Brian Hewitt, piped up and said no-one in Australia was ever “forced” to be vaccinated.
Senator Hansen took exception to the comment and asked if Hewitt would retract his statement.
Hewitt held his position saying, “No. I believe firmly that nobody was forced to have a vaccine.”
“A lot of Australians will disagree with you on that one,” retorted Senator Hansen.
Senator Matt O’Sullivan was incredulous. He said that in his state of Western Australia, there were mandates across the board, with “very, very few exceptions.”
“If you wanted to go to work, and earn a living and provide for your family, you had to be vaccinated. I am staggered that that was your response to questions in relation to whether or not people were forced to have vaccines,” said O’Sullivan.
Many of O’Sullivan’s constituents had to go without income because the state government was “forcing” them to be vaccinated against their will.
Hewitt looked down to read a pre-prepared answer, much to the dismay of listeners.
“Senator, mandates, and vaccine requirements are determined by governments. As a company we were not involved in any government vaccine mandates. I don’t believe the mandates actually forced individuals to get vaccinated.”
Pfizer did confirm that it enforced a vaccine mandate within its own company and that it had imported a special batch of covid-19 vaccines for its employees. Why the special batch? “So that no vaccine would be taken from government stocks,” said Hewitt.
Thiru also said there were some exemptions for medical or religious reasons and that “a small number of colleagues departed the company,” presumably because they did not comply with the mandate.
Moderna, on the other hand, distanced itself from commenting on vaccine mandates.
Clarke, Director, Scientific Leadership, Moderna.
Moderna’s Vice President of Medical Affairs Jane Leong said, “We do not have a view on decisions taken by public health agencies or governments in relation to vaccine mandates. This is purely a matter for policymakers.”
At the finish line, Pfizer and Moderna executives managed to expertly dodge questions, they couldn’t recall their own rate of SAEs, they wouldn’t admit that covid vaccines cannot stop transmission, and they refused to divulge details of their indemnity agreements with the government.
Responses to questions on notice are due Aug 17, 2023.
The sky is falling, the sky is falling, no just another climate loon ignoring Science. No my friends the world isn’t ending and glaciers will continue to break off just as they have since the beginning of time.
PBS producers ran soundbites of seven souls who claimed the fear of “climate change” had made them anxious about the future, including Mark Ikeda, who said: “Climate anxiety affects my daily life, by the decisions I make about when I want to go someplace or where I want to go or more [inaudible], how I want to travel.”
John Yang interviewed Leslie Davenport, who is a “climate psychology therapist.” She says,” We view distress, upset, sadness, grief, anger about climate change to be a really reasonable, even healthy reaction.” She referred to this field of psychology as “emerging.” One has to ask, is climate change even qualify as science?
WATCH:
Video and partial transcription courtesy of NewsBusters
This is a clown who served during the Obama administration. Thought the job was all fun and games. Much of this article is Government misinformation. But there are parts that they get right. Come 2024 all these clowns that took part in the attacks on our young and elderly will be gone or in jail.
FDA Head Robert Califf Battles Misinformation — Sometimes.
Robert Califf, MD, the head of the FDA, doesn’t seem to be having fun on the job.
“I would describe this year as hand-to-hand combat. Really, every day,” he said at an academic conference at Stanford in April. It’s a sentiment the FDA commissioner has expressed often.
What’s been getting Califf’s goat? Misinformation, which gets part of the blame for Americans’ stagnating life expectancy. To Califf, the country that invents many of the most advanced drugs and devices is terrible at using those technologies well. And one reason for that is Americans’ misinformed choices, he has suggested. Many don’t use statins, vaccines, or COVID-19 therapies. Many choose to smoke cigarettes and eat the wrong food.
Califf and the FDA are fighting misinformation head-on. “The misinformation machine is really causing a lot of death,” he said, in an apparent ad-lib, this spring in a speech at Tufts University. The pandemic, he told KFF Health News, helped “crystallize” his need to tackle misinformation. It was a “blatant case,” in which multiple studies gave evidence about very effective therapeutics against COVID. “And a lot of people chose not to do it.” There were “large-scale purveyors of misinformation,” he said, poisoning the well.
Occasionally, though, Califf and the FDA have added to the cacophony of misinformation. And sometimes their misinformation is about misinformation.
Califf hasn’t been able to consistently estimate misinformation’s public health toll. Last June, he said it was the “leading cause of meaningful life-years lost.” In the fall, he told a conferenceopens in a new tab or window: “I’ve been going around saying that misinformation is the most common cause of death in the United States.” He continued, “There is no way to prove that, but I do believe that it is.”
At other times, as in April, he has called the problem the nation’s “leading cause” of premature death. “I’ll keep working on this to try and get it right,” he said. Later, in May, he said, “Many Americans die or experience serious illness every year due to bad choices driven by false or misleading information.”
Several factors are at the root of those differences. But Americans’ choices, often informed by bad or misleading data, political jeremiads, or profit-seeking advertising, are among the causes. For instance, one 2023 paper estimated that undervaccination against COVID — caused in part by misinformation — costs as much as $300 million per dayopens in a new tab or window, accounting for both the costs of healthcare and economic costs, like missed work.
Outside experts are sympathetic. Misinformation is a “huge problem for public health,” said Joshua Sharfstein, MD, a Johns Hopkins University public health professor and former FDA principal deputy commissioner. Having a strategy to combat it is crucial. But, he cautioned, “that’s the easiest part of this.”
The agency, which regulates products that consumers spend 20 cents of each dollar on per year, is putting more muscle behind the effort. It’s begun mentioning the subject of misinformation in its procurement requests, like one discussing the needopens in a new tab or window to monitor social media for misinformation related to cannabis.
Califf has noted small victories. Ivermectin, once touted as a COVID wonder drug, “eventually” became one such win. But, then again, its use is “not completely gone,” he said. And, despite winning individual battles, his optimism is muted: “I’d say right now the trend in the war is in a negative direction.”
Some of those battles have been quite small, even marginal.
And it’s difficult to know what to take on or respond to, Califf said. “I think we’re just in the early days of being able to do that,” he told KFF Health News. “It’s very hard to be scientific,” he said.
Take the agency’s experience last fall with “NyQuil chicken” — a purportedly viral cooking trend in which users roasted their birds in the over-the-counter cold medicine on social media platforms like TikTok.
Califf said his agency’s “skeleton crew” — at least relative to Big Tech giants — had picked up on increasing chatter about the meme.
But independent analyses don’t corroborate the claim. It seems much of the interest in it came only after the FDA called attention to it. The day before the agency’s pronouncement, the TikTok app recorded only five searches on the topic, BuzzFeed Newsfound in an analysis of TikTok dataopens in a new tab or window. That tally surged to 7,000 the week after the agency’s declaration. Google Trends, which measures changes in the number of searches, shows a similar pattern: Interest peaked on the search engine in the week after the agency announcement.
Califf also claimed “injuries” occurred to participants “directly” due to the social media trend. Now, he said, “the number of injuries is down,” though he couldn’t say whether the agency’s intervention was the cause.
Again, his assertions have fuzzy underpinnings. It’s not clear what, if any, actual damage the NyQuil chicken fad caused. Poison control centers don’t keep that data, said Maggie Maloney, a spokesperson for America’s Poison Centers. And, after multiple requests, agency spokespeople declined to provide the FDA’s data reflecting increased social media traffic or injuries stemming from the meme.
In countering misinformation, FDA also risks coming off as high-handed. In September 2021, the agency tweeted about purported mythsopens in a new tab or window and misinformation on mammograms. Among the myths? That they’re painfulopens in a new tab or window. Instead, the agency explained that “everyone’s pain threshold is different” and the breast cancer-screening procedure is more often described as “temporary discomfort.”
Statements like these “erode trust,” said Lisa Fitzpatrick, MD, MPH, MPA, an infectious diseases physician and currently the CEO of Grapevine Health, a startup trying to improve health literacy in underserved communities. Fitzpatrick has previously served as an official with the District of Columbia’s Medicaid program and with the CDC.
“Who are you to judge what’s painful?” she asked, rhetorically. It’s hard to brand subjective impressions as misinformation.
Califf acknowledged the point. Speaking to 340 million Americans is difficult. With mammograms, the average patient might not have a painful experience — but many might. “Getting across that kind of nuance and public communication, I think, is in its early phases.”
Scrutiny over the agency’s role regarding food and nutrition is also mounting. After independent journalist Helena Bottemiller Evich wrote an article criticizing the agency for relying on voluntary reporting standards for baby formula, Califf tweeted to correctopens in a new tab or window a “bit of misinformation,” saying the agency did not have such authority.
An agency communications specialist made a similar intervention with New York University professor Marion Nestle, PhD, MPH, referring to a “troubling pattern of articles with erroneous information that then get amplified.” The agency was again seeking to rebut arguments that the agency had erred in not seeking mandatory reporting.
“As I see it, the ‘troubling pattern’ here is FDA’s responses to advocates like me who want to support this agency’s role in making sure food companies in general — and infant formula companies in particular — do not produce unsafe food,” Nestle retortedopens in a new tab or window. Notwithstanding the agency’s protests to Evich and Nestle, the agency had only recently asked for such authority.
Efforts to respond to or regulate misinformation are becoming a political problem.
In July, a federal judge issued a sweeping, yet temporary, injunctionopens in a new tab or window — at the instigation of Republican attorneys general, multiple right-wing political groups, and prominent anti-vaccine advocate Robert F. Kennedy Jr.’s Children’s Health Defense — barring federal health officials from contacting social media groups to correct information. A large section of the ruling detailed efforts by a CDC official to push back on suspected misinformation on social media networks.
An appeals court later issuedopens in a new tab or window its own temporary ruling — this time countering the original, sweeping order — nevertheless underscoring the extent of pushback on government pushback against misinformation. Califf has consistently played down the government’s ability to solve the problem. “One hundred percent of experts agree, government cannot solve this. We have too much distrust in fundamental institutions,” he said last June.
It’s a remarkable change from his previous tenure leading the agency during the Obama administration. “I would describe the Obama years as genteel, intellectual, and a lot of fun,” he has said. Now, however, Califf is bracing for more misinformation. “It’s just something that I think we have to come to grips with,” he told KFF Health News.
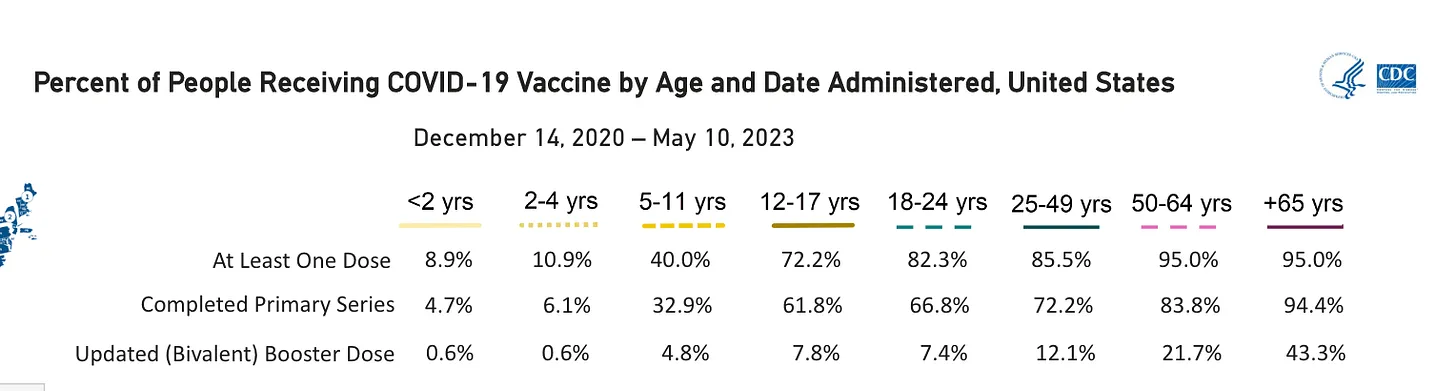
Just look at the rates of booster administered. This must be causing some heartburn among the public health administrative set.
Concentrating on the pediatric population (kids)…
In babies and kids up to four years old, only 0.6% are fully vaccinated. About 5% have completed the primary series and 9% to 11% have had at least one dose.
The 5-11 year olds also are no longer getting vaccinated. Less than 5% have had a booster and only 33% have completed the 2-shot series.
It is believed that not being able to do extracurricular activities without vaccination, caused the 12-17 year olds to get vaccinated. But the good news is that only 8% have been boosted.
Frankly, these numbers are extraordinary. Parents are no longer vaccinating with this experimental vaccines.
The vast majority of adults have not had a booster!
I think we all deserve a big thanks for spreading the message. This is a world-wide group effort to fight big pharma and big government(s) controlling the narrative and we are winning!
The Five Eyes Alliance must be gritting their teeth!
Last Friday, the International Agency for Research on Cancer (IARC), which is part of the World Health Organization, classified aspartame, a non-nutritive sweetener widely used in diet sodas, as “possibly carcinogenic to humans.” Other substances that share the designation include gasoline, diesel fuel, engine exhaust, chloroform, DDT, and lead. But despite aspartame’s inclusion among that ominous cadre of chemicals, you can continue drinking diet sodas almost entirely worry-free. Here’s why.
IARC is terrible at science communication
IARC’s cancer classifications may be one of the greatest failures of science communication in the world. The agency reports “hazard” (that is, whether a substance could be dangerous) rather than “risk” (that is, the magnitude of any potential danger). By declaring aspartame as “possibly carcinogenic,” people around the world interpret that message as, “Diet sodas are causing cancer.” As always, context is everything, and IARC’s designations mostly leave that out.
Numerous studies over the years have probed whether aspartame is linked to a higher risk of cancer. The resulting data is essentially a wash. Some studies found a small increased risk, while others found no correlation. Trials in rodents do show that consuming inordinately large amounts of aspartame can cause cancer, but this is true for many chemicals eaten in extreme excess. That’s why the Joint FAO/WHO Expert Committee on Food Additives (JECFA) reasonably warns people against consuming more than 40 milligrams of aspartame per day per kilogram of body weight. For a 200-pound person, that’s equivalent to drinking 18 cans of diet soda.
“And even this ‘acceptable daily intake’ has a large built-in safety factor,” Sir David Spiegelhalter, an emeritus professor of statistics at the University of Cambridge, told the Science Media Center. In other words, the 40 mg/kg/day guideline is a conservative estimate; you could probably consume much more and be just fine. In fact, the JECFA considered the same evidence on aspartame and cancer that IARC did and concluded that the evidence for a link is not convincing, an opinion shared by the U.S. Food and Drug Administration.
Obesity risk vs. cancer risk
The IARC’s classification of aspartame as a possible carcinogen undoubtedly will cause a PR headache for food companies utilizing the compound, and perhaps prompt them to reformulate their products to avoid the risk of opportunistic lawsuits. The move unfortunately also may lead drinkers of diet sodas to choose sugar-laden options instead. Physician Walter Willett of the Harvard T.H. Chan School of Public Health told NPR that would be the “worst possible decision.” The health consequences of consuming large amounts of added sugar — including diabetes and obesity — dwarf the remote cancer risk from aspartame.
The simple truth is that every decision in your life affects your risk of cancer, from how much you sleep, to what you eat for breakfast, to whether you ride your bike or drive to work. How we balance that equation is up to each of us. Some decisions, like smoking and using tanning beds, increase the risk of cancer dramatically. Others, like eating right and exercising, clearly lower it. Many more, like using aloe vera, eating pickled vegetables, and drinking diet sodas, have such a small effect — if any — that it’s not really worth worrying about.
Leonard Ortiz/MediaNews Group/Orange County Register via Getty Images
Getting back at the junk science. In-N-Out Requiring Employees to Show Medical Note to Wear Masks. Who can forget the COVID days when the loons told you that you bascially needed an exemption from Congress to not wear a mask? Or about 50,000 medical doctors approved by Tony the Fauch to not wear a mask? OK I’m stretching it.
Well In-N-Out Burger has loon employees who still think that they’re gonna die if they don’t wear a mask at work. Crazy I know. So In-N-Out wants those workers to have a doctors excuse saying why they have to mask up.
“It stipulates that no employee may wear a mask unless they provide a medical note that exempts them from the requirement. If they provide the medical note, they must wear a company-provided N-95 mask unless they can produce another note exempting them from that requirement too,” it added
Discovering the disinformation playbook An excerpt from ‘The War on Ivermectin: The Medicine That Saved Millions and Could Have Ended the Pandemic’, by Dr. Pierre Kory
Having fought in the “War on Ivermectin” now for almost two and half years, I know most of the military plays. But when I first set foot on the battlefield, I was blissfully unaware of the rules of engagement. Hell, I didn’t even know I was fighting in a war.
One thing was crystal clear to me: Something illicit was happening around ivermectin, and Big Pharma’s fingerprints were all over the crime scene. But in the beginning, I truly believed that the pandemic would be over in a matter of months—just as soon as our review paper was published. The world would know that there was an incredibly effective agent to prevent and treat Covid-19; deaths would stop, and life would resume.
It physically pains me to write that last sentence.
I credit my combat training to two people, both of whom appeared in my life around the same time. The first was a man who writes under the pen name Justus Hope, MD, author of Ivermectin for the World. I had come across his book as well as multiple articles published in a California newspaper called The Desert Review in my research, so I knew who he was when he reached out. We had several in-depth conversations during which he explained his long-standing interest in Big Pharma’s war on repurposed drugs. That interest was triggered by a close friend with brain cancer which led him to the discovery that there were multiple effective repurposed drugs to treat cancer that had long been suppressed by Big Pharma. Early in the pandemic, he published a book called Surviving Cancer, Covid-19, and Disease: The Repurposed Drug Revolution. I was beginning to understand that this was an old, old war.
My second mind-altering mentor during this period was a complete stranger named Bill Grant, PhD, a physicist and the founder and president of the Sunlight, Nutrition, and Health Research Center in San Francisco. Bill is also one of the world’s foremost experts on the science behind vitamin D, with more than 300 peer-reviewed papers to his name. Out of the blue, Bill reached out to me in March of 2021 with a simple, two-line email:
Dear Dr. Kory, What they are doing to ivermectin they have been doing to Vitamin D for decades. Bill
The note was followed by a link to an article by a group of scientists detailing precisely how disinformation is used to sway public opinion. Intrigued, I clicked the link.
The article described various disinformation tactics by equating them to American football plays. By the time I got to the end of that article, a switch inside me had flipped. I instantly knew that it was the key to understanding a world that I no longer recognized.
The article went on to detail five primary disinformation “plays” or tactics used by companies or industries when science emerges that is inconvenient to their interests: the fake, the fix, the blitz, the diversion, and the screen. As I read, I could think of dozens of examples for every single one of those maneuvers that had occurred around ivermectin since my senate testimony had gone viral.
The mother of all Macy’s 4th of July fireworks celebrations was going off in my brain; one realization exploding after another, each one brighter and more astonishing than the last.
Holy crap. The FLCCC was in the middle of a disinformation war with the pharmaceutical industry.
From that day on, that conceptual framework was the only thing that could make sense of what had happened and what was yet to happen in my attempts to highlight one of the safest and most effective treatments in any disease in history.
Although each play was widely represented in the events surrounding the Covid response, “the fake” was by far the most prominent—and the most damaging. In regard to repurposed drugs specifically, it involves conducting trials “designed to fail,” selectively publishing negative results while censoring positive results, and planting negative ghost-written editorials in legitimate journals. The article emphasized that these tactics can gravely undermine public health and safety.
You don’t say.
“The fake” formed the foundation of a campaign that would result in one of the most significant humanitarian catastrophes in history, causing millions of deaths around the world.
To be clear, ivermectin wasn’t the first casualty of World War Covid. The same tactics had been used against hydroxychloroquine (HCQ) in 2020 and had they not, HCQ would have been deployed at the onset of the pandemic and saved even more lives. The closest and best description of that war I’ve discovered was featured in Robert F. Kennedy’s The Real Anthony Fauci (Skyhorse Publishing, 2021), a brilliant, expertly researched, and undeniably incriminating takedown of “America’s Doctor.”
“HHS’s early studies supported hydroxychloroquine’s efficacy against coronavirus since 2005, and by March 2020, doctors from New York to Asia were using it against Covid with extraordinary effect,” Kennedy wrote. By autumn, more than 200 studies supported treatment with hydroxychloroquine. “From the outset, hydroxychloroquine and other therapeutics posed an existential threat to Dr. Fauci and Bill Gates’ $48 billion Covid vaccine project, and particularly to their vanity drug remdesivir, in which Gates has a large stake. Under federal law, new vaccines and medicines cannot qualify for Emergency Use Authorization (EUA) if any existing FDA-approved drug proves effective against the same malady.”
In other words, if HCQ or ivermectin had been recognized as a viable treatment, the massive cash cow that was the global Covid-19 vaccine campaign would have been slaughtered on the spot.
Keep in mind that HCQ and ivermectin not only threatened the vaccine campaign, but also the massive and exploding competitive market for other pricey Big Pharma products like Veklury (commonly known by its generic name, remdesivir), Paxlovid, molnupiravir, and monoclonal antibodies. Never in history had two generic, repurposed medicines threatened a marketplace of such a colossal size.
The answer to that pesky little conundrum?
Disinformation.
Over and over, each devious play has been strategically deployed to further the interests of the establishment to the unbridled disservice of mankind.
You can find ‘The War on Ivermectin: The Medicine That Saved Millions and Could Have Ended the Pandemic’ at a bookstore near you.
Someone (who needs to remain anonymous) was able to obtain the death certificates from Minnesota for all deaths that occurred from 2015 to the present, which presented the opportunity to see if the CDC is being entirely honest about the US death data. Unsurprisingly, the CDC is not.
As we shall document, the CDC is concealing references to a covid vaccine on Minnesota death certificates (that are exceedingly rare to begin with because of widespread medical establishment denialism of vaccine adverse side effects). In almost every death certificate that identifies a covid vaccine as a cause of death, the CDC committed data fraud by not assigning the ICD 10 code for vaccine side effects to the causes of death listed on the death certificate.
Background
When someone dies, there is a death certificate that is filled out for official/legal purposes. Death certificates contain a lot of information (some states include more than others), including the causes of death (CoD).
Causes of death refer to the medical conditions that ultimately played some role in the demise of the decedent. To qualify as a CoD, a condition only needs to contribute to the medical decline of the decedent in some way, but doesn’t have to be directly responsible for whatever ultimately killed the person. If someone had high blood pressure, and subsequently suffered a heart attack that led to cardiac arrest which killed them, all three conditions qualify as CoD. On the other hand, this unfortunate fellow’s ingrown toenail is not a cause of death, because it in no way contributed to their demise.
This is from the CDC’s own guidance explaining how to properly fill out CoD’s on a death certificate (you don’t need to understand the difference between Cause A, B, etc, for this article):
The critical thing to keep in mind is that the person filling out the death certificate writes a text description of the CoD’s, but doesn’t assign the ICD 10 codes for the CoD’s.
That’s the CDC’s job.
ICD 10 Coding System for CoD’s
There is a fancy coding system that is used to classify the many thousands of medical conditions that can play a role in death known as the International Classification of Diseases. Every few years, it is updated/revised to keep up with new medical (or bureaucratic) developments as new conditions are discovered, and old conditions are reorganized or reclassified.
The current iteration of the ICD used for the deaths we’re looking at is the ICD 10 (the 10th version). It is basically a hierarchical classification system:
There are codes for practically every random weird thing you can think of:
There are codes for practically every random weird thing you can think of:
These are categories themselves – a code can go as 7 characters long:
(There are other ICD 10 codes for various specific complications or side effects of vaccines, but the point remains that an ICD 10 code for vaccine side effects exists.)
CDC – Centers for Data Concealment
The CDC receives the death certificates from the various states and applies ICD 10 codes. This is primarily done with a secret algorithm, with a tiny percentage of cases adjudicated by CDC staff when the algorithm is unable to confidently assign an ICD code to the text description written on the actual death certificate (such as confounding spelling or a text description that does not make much sense). I confirmed this with a biostatistician who works for a DoH in a US state (I’m leaving out which one because I want to preserve my persona grata status). The individual who obtained the MN death certificates likewise confirmed with state officials that the ICD codes in their data were assigned by the CDC.
What a death certificate identifying a covid vaccine as a CoD *should* look like
There are three death certificates in the MN tranche that contain either T88.1 or Y59.0. One is for a flu vaccine reaction, and – surprisingly – the other two are for a covid vaccine.
Note – when used below:
UCoD (Underlying Cause of Death) refers to “the disease or injury that initiated the train of events leading directly to death, or the circumstances of the accident or violence which produced the fatal injury.”
MCoD (Multiple Causes of Death) refers to “the immediate cause of death and all other intermediate and contributory conditions listed on the death certificate.” (everything else)
The first death certificate contains a covid vaccine ICD (below), and it looks like the CDC was trapped and could not avoid putting it on without fundamentally rewriting the death certificate, because the vaccine complication is unambiguously listed as the UCoD (this death certificate is saying the person was killed by a heart attack caused by the covid vaccine within minutes of injection):
The second death certificate the CDC deigned to assign a vaccine ICD (and not only one but *BOTH* vaccine ICD codes(!!)) feels like perhaps a rogue CDC employee was working that day and snuck it in:
In any event, as we can clearly see, both T88.1 and Y59.0 are indeed appropriate for when a covid vaccine is listed as a CoD. Thus the CDC cannot claim that there was no official ICD 10 code that could be used to designate covid vaccines (or any other excuse).
The FRAUD:
With that introduction, below are 7 death certificates from Minnesota that identify a covid vaccine as a cause of death where the CDC omitted the corresponding ICD 10 code identifying a vaccine side effect when the CDC assigned ICD codes to the death certificates.
The first fraudulently filled out death certificate offers a crucial detail highlighting not only the fraud but the naked double standards for assigning CoD’s.
This death certificate identifies both a covid vaccine and covid itself as contributory CoD’s (in the last row highlighted in yellow, vaccine underlined in green, covid in blue):
“covid vaccine second dose 10 hrs prior to death”
“history of covid infection in May 2020” (about 7-8 months prior to death)
Any remotely objective person would presume that if a condition that occurred 7 months prior without any clear link to the actual death still nevertheless meets the standard for being identified as a CoD, then surely a condition or event that occurred a mere TEN HOURS before death identified by the doctor filling out the death certificate merits inclusion as a CoD.
Yet, the CDC assigned U70.1 – “COVID-19, virus identified” – for covid, but neglected to assign T88.1 or Y59.0 for the covid vaccine.
A second point to highlight is that we see that anything mentioned as a CoD, even in the context of “history of” that had (presumably) been long resolved, is a legitimate CoD insofar as assigning an ICD 10 code and epidemiological data are concerned.
This decedent suffered a cardiac arrest that ultimately led to her death *ONE DAY* after being vaccinated.
(For the record, I am not bothered by the “though it’s not clear as to any mechanism for how the vaccine could have led to the cardiac arrest” line. This death occurred February 24, 2021 – well before there was any sort of public awareness about the multiple plausible mechanisms by which the vaccine could cause heart damage. So to me, whoever filled out the death certificate was a gutsy fellow willing to identify a covid vaccine on a death certificate that had his name on it.)
Fraudulent Death Certificate #3
This death certificate doesn’t merely identify a covid vaccine, it explains that the decedent “felt sick after the vaccine” and died 4 days later from a heart attack.Yet, no T88.1 or Y59.0.
This death certificate provides that the decedent received her second dose of Pfizer 18 days prior to her death.
Here we have a 65-year-old male who was killed by a heart attack 12 days after getting vaccinated.
This case is especially noteworthy. Someone involved with this death informed me that the family had to pressure the coroner to put the recent covid booster on the death certificate. A family member also filed a VAERS report themselves, after the patient’s doctors declined to do so.
Furthermore, the CDC applied W34 as the UCoD. What is W34 for?
‘accidental discharge and malfunction from other and unspecified firearms and guns.’
There is no mention of any firearms mishaps on the death certificate.
One would have to wonder how such an errant code came to be, especially on a death certificate that contains other ICD 10 shenanigans. It is unlikely that ‘Y590’ or ‘T881’ would be ‘misspelled’ or algorithmically mixed up with ‘W34.’
Perhaps if there were no other instances of fraudulent omittance of vaccine ICD codes on other death certificates, and the CDC wasn’t in the habit of routinely assigning U07.1 for a covid infection that resolved a year ago, the failure to include T88.1 or Y59.0 here could be excused.
At minimum, this death certificate should contain T88.0 – ‘Infection following immunization’ – to document the breakthrough infection (which is a subject for a separate article as this seems to be fairly widespread).
Additional Observations
The following table shows the date of death and age for all 9 death certificates shown above that identified a covid vaccine as a CoD:
It is striking that 7/9 died before May 2021. This is odd – if anything, the deaths should skew later, not earlier. Vaccine adverse events were denied – with maximum prejudice and then some – for many months before the medical mainstream has finally (begrudgingly) started to acknowledge that the covid vaccines can trigger potentially lethal pathologies (in exceedingly rare instances to be sure).
The clustering of death certificates mentioning a covid vaccine at the beginning of the rollout suggests that ‘administrative’ interference likely played a role in discouraging coroners from mentioning a covid vaccine on death certificates.
Another noteworthy tidbit here is the age of the decedents: every single one is a senior citizen, and the average age of the decedents is 80. This is important to highlight because whereas young people “dying suddenly” stands out, there has been much less attention or acknowledgement of the covid vaccine’s devastating toll upon the old and frail, where deaths – even those that occur in close proximity to vaccination – are readily attributed to prior health conditions.
Finally, the actions of the CDC call into question whether the CDC is altogether qualified or trustworthy enough to be the steward of the nation’s epidemiological data. The CDC manages many of the datasets that underpin whole fields of study. If the CDC is willing to fraudulently alter data (or even if the CDC is just too incompetent to avoid corrupting data), all data under the aegis of the CDC is potentially suspect, especially if it relates to a controversial political or social issue. The implications of this are disturbing, to say the least.