
Did Norfolk Southern neglect safety protocols in pursuit of DEI and ESG initiatives?
On February 3rd, dozens of Norfolk Southern train cars derailed while traveling through East Palestine, Ohio, with 11 of those cars carrying ultra hazardous chemical agents. Some three days later, those chemicals were burned off into the air, after officials expressed concerns that the materials could explode and ignite an even greater catastrophe. Could all of this have been avoided?
On Thursday, the NTSB (National Transportation Safety Board) determined in a preliminary report that an overheated wheel bearing on a Norfolk Southern train car could be responsible for the derailment that occurred.
The report listed multiple operational concerns, adding that “surveillance video … showed what appeared to be a wheel bearing in the final stage of overheat failure moments before the derailment.” This seems to indicate that this was a disaster that could’ve been avoided with proper safety protocols in place.
We are offered clues of possible neglect in Norfolk Southern’s 2022 ESG (environmental, social, and corporate governance) report, which showcases how the railway corporation has completely embraced the modern “stakeholder capitalism” agenda that inundates seemingly every major American corporation.


The report, published in late 2022, highlights how Norfolk is pursuing wokeness and the climate agenda over safety and merit-based hiring.
It contains a message from Alan Shaw, the rail company’s CEO, who has been in the news lately for all of the wrong reasons. In a letter to readers, Shaw proudly announced that they would continue “reducing our carbon footprint” while expanding their DEI (Diversity, Equity, and Inclusion) initiatives.
Shaw, by the way, failed to show up for the latest community meeting on the railway disaster on Thursday.

As for the DEI page, it touts how Shaw signed the “CEO Action for Diversity and Inclusion pledge,” a product of the ultra woke consulting firm PricewaterhouseCoopers.
The pledge commits employers to pursue “racial equity” in their hiring processes and “implement and expand unconscious bias education and training.” In short, follow the agenda and you will be rewarded by The System.
In its DEI page, Jason Pettway, the company’s Vice President for Diversity, Equity and Inclusion (a role created by the company in 2021) cheers the fact that more than half of all new hires belong to a racial minority.
The DEI page makes clear to readers that Norfolk is committed to hiring its workforce on the basis of gender and skin color, and not merit.
Forget about the mushroom cloud and toxic gasses they helped to launch over East Palestine. In its ESG section, Norfolk Southern has won plenty of awards recently for “delivering the low-carbon economy.”
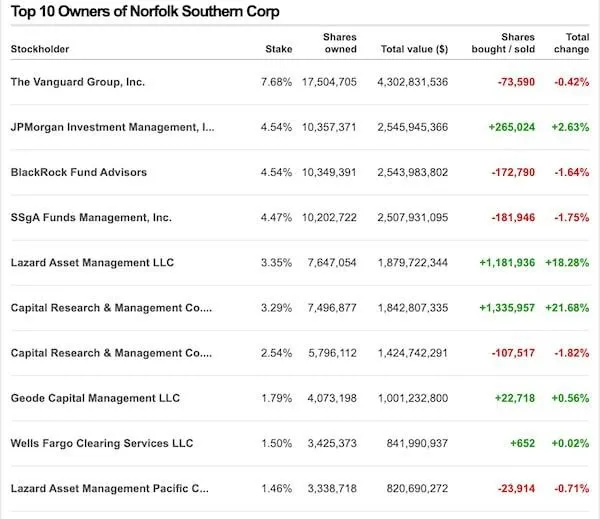
Did all of this “climate leadership” mean Norfolk Southern was cutting corners on safety standards? The report was surely celebrated by Norfolk’s multi-trillion dollar asset management behemoth stakeholders.
As for the people of East Palestine, Ohio, they are left with the wreckage in their physical backyards, and with a series of questions that remain unanswered from Norfolk Southern officials, who have largely refused to hold themselves accountable for the consequences of their failures.






















