And no accountability or justice is forthcoming.

The estimated deaths from the COVID crisis are probably around ten million people or more
The World Health Organization estimates that (worldwide) there have been 763,740,140 confirmed cases of COVID-19, including 6,908,554 deaths as of April 19, 2023. This does not include additional components of the excess mortality during the COVID crisis being documented by many in Western nations, for which scientists and the various governments seem to not know what the causative agent is, and no government seems to want to investigate… Although most will agree privately that these deaths are also related to COVID-19 “public health” policies in some way or another. These include deaths from lockdowns (famine, suicide, violence, alcohol, and drug abuse), long COVID, vaccine deaths, lack of medical care for cancer and other diseases, etc. All told the estimated deaths from the COVID crisis are probably around ten million people or more. Ten million people is a very big number. It is hard to even fathom.
For comparison, the largest natural disaster (excluding famine) of the 20th century was the Chinese Yangtze River Floods in 1931, which killed 3.7 million people both directly and indirectly, with many people dying from poor sanitation and diseases. In 1958, the Chinese Yellow River Flood killed around a million people, although estimates widely vary. Other floods, cyclones, earthquakes all killed countless people. But none did so with as much devastation to human life as was done by the SARS-CoV-2-WIV virus.
This disaster was man-made!
But we also know this was not a natural disaster; this disaster was man-made.
A list of genocides on Wikipedia shows that there have been no single human atrocities in the history of mankind that have come close to the deaths caused from the COVIDcrisis.
How do we “know this”? Because we have the receipts thanks to Judicial Watch, as well as the Congressional investigations – still ongoing.
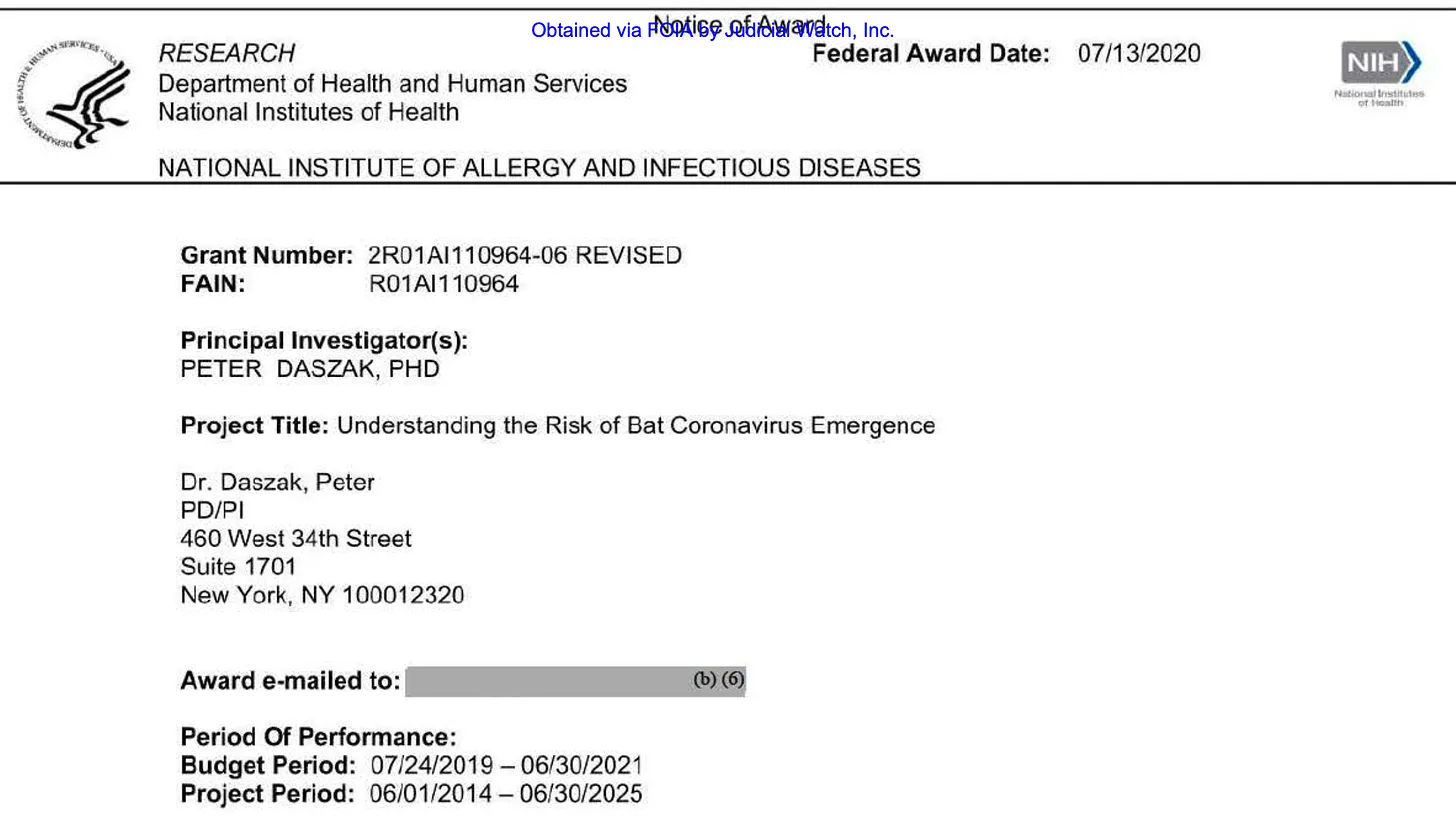
This week, Judicial Watch received 552 pages from the U.S. Department of Health and Human Services (HHS). These documents include the initial grant application, biosketches, budgets and annual reports to the NIH from EcoHealth Alliance. They describe the specific aims of the project, which include creating mutant viruses SARS (and MERS viruses) “to better predict the capacity of our CoVs [coronaviruses] to infect people.”
I spent the afternoon reading these documents and the 552 pages are a gold mine of information. But the specific aim 3 of the contract is particularly important. It reads in full:
Specific Aim 3: Testing predictions of CoV inter-species transmission. We will test our models of host range (i.e. emergence potential) experimentally using reverse genetics, pseudovirus and receptor binding assays, and virus infection experiments in cell culture and humanized mice. With bat-CoVs that we’ve isolated or sequenced, and using live virus or pseudovirus infection in cells of different origin or expressing different receptor molecules, we will assess potential for each isolated virus and those with receptor binding site sequence, to spill over. We will do this by sequencing the spike (or other receptor binding/fusion) protein genes from all our bat-CoVs, creating mutants to identify how significantly each would need to evolve to use ACE2, CD26/DPP4 (MERS-CoV receptor) or other potential CoV receptors. We will then use receptor-mutant pseudovirus binding assays, in vitro studies in bat, primate, human and other species’ cell lines, and with humanized mice where particularly interesting viruses are identified phylogenetically, or isolated. These tests will provide public health-relevant data, and also iteratively improve our predictive model to better target bat species and CoVs during our field studies to obtain bat-CoV strains of the greatest interest for understanding the mechanisms of cross-species transmission.
Later, they write (page 195):
we will assess potential for each isolated virus and those with receptor binding site sequence, to spill over. We will do this by sequencing the spike (or other receptor binding/fusion) protein genes from all our bat-CoVs, creating mutants to identify how significantly each would need to evolve to use ACE2, CD26/DPP4 (MERS-CoV receptor) or other potential CoV receptors.
It is important to understand that, although these quotes are technical and well beyond many to understand, the bottom line is that this project was and is gain of function research. In contrast to Dr. Fauci’s sworn testimony to Congress.
It is important to pull out these sections highlighting the gain of function research conducted that led to the deaths of millions of people. This is the only way I know of to make scientists, the courts and policy makers aware that this is not a conspiracy theory. This is real. That these deaths were caused by manslaughter.

The only question now is was this an accidental or intentional release of the man-made virus? Was it manslaughter or murder?
According the 552 pages released, the Wuhan Institute of Virology was so safe, there were assurances made to this effect and the facilities were never inspected by the US government. The risk of mutant viruses escaping the laboratory was never even discussed in the risks associated with conducting this research.
If it was so safe, doesn’t the intentional release of this mutant virus have to be considered?
This only gets worse. The year 2 report (2016) clearly states that AIM 3 for year 3 had been expanded to also include conducting gain-of-function research using the MERS virus!
Specific Aim 3: Testing predictions of CoV inter-species transmission. The following experiments will be undertaken in Year 2 (page 197)
-An infectious clone of full-length MERS-CoV will be constructed using reverse genetic method. Using the S sequence of different MERS-related viruses identified from Chinese bats, the chimeric viruses with S gene of bat MERS-related coronaviruses and backbone of the infectious clone of MERS-CoV will be constructed to study the receptor usage and infectivity of bat MERS-related coronavirus.
The MERS virus (MERS-CoV) is highly pathogenic. During the 2012 outbreaks, there were about 2,500 known cases and 800 deaths. If these numbers are correct, this would be a case fatality rate of 31%! MERS-CoV did not appear to be highly infectious, unlike SARS-CoV-2-WIV (the virus created by Ralph Baric/EcoHealth/WIV).
Note that the above passage includes references to creating new chimeric variants and linking them to the infectivity of MERS! Could you imagine if they also created a more highly infectious MERS virus, that they spread through out the world, like SARS-CoV-2-WIV? The devastation would be like nothing the world has ever seen.
Moving on to the 2017 report (page 253):
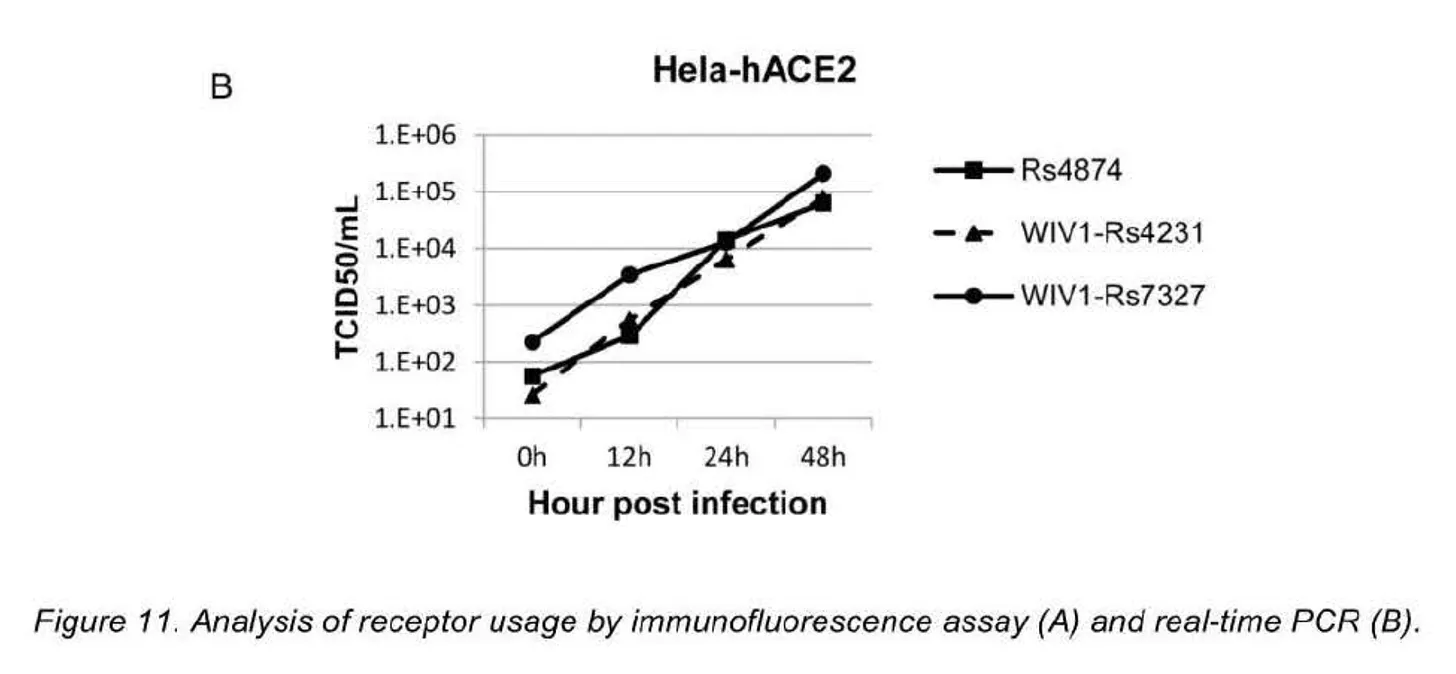
In Year 3, we successfully isolated Rs4874 from the single fecal sample. Using the reverse genetic system we previously developed, we constructed two chimeric viruses with the WIV1 backbone replaced with the S gene of Rs7327 and Rs4231, respectively. Vero E6 cells were respectively infected with Rs4874, WIV1-Rs4231S and WIV1- Rs7327S, and efficient virus replication was detected by immunofluorescence assay in all infections. To assess the usage of human ACE2 by the three novel SL-CoVs, we conducted virus infectivity studies using Hela cells with or without the expression of human ACE2. All viruses replicated efficiently in the human ACE2-expressing cells. The results were further confirmed by quantification of viral RNA using real-time RT-PCR (Fig.11).
The full-length infectious eDNA clone of MERS-CoV has been successfully constructed. The full-lengthS gene of 12 different novel bat MERS-related coronaviruses have been amplified and cloned into the T-vectors. In Y4, we aim to use the reverse genetic method, and construct chimeric viruses with the backbone of MERS-CoV and the S genes from diverse newly identified bat MERS-related coronaviruses, to examine the pathogenicity of bat MERS-related coronaviruses on cell and animal levels.
More gain of function research.
Moving on to Year 4 (page 275):
Specific Aim 3: Testing predictions of CoV inter-species transmission.
In Vivo Infection of Human ACE2 (hACE2) Expressing Mice with SARSr-CoV S Protein variants
Using the reverse genetic methods we previously developed, infectious clones with the WIV1 backbone and the spike protein of SHC014, W IV16 and Rs4231, respectively, were constructed and recombinant viruses were successfully rescued. In Year 4, we performed preliminary in vivo infection of SARSr-CoVs on transgenic mice that express hACE2. Mice were infected with 105 pfu of full-length recombinant virus of WIV1 (rWIV1)and the three chimeric viruses with different spikes. Pathogenesis of the 4 SARSr-CoVs was then determined in a 2-week course. Mice challenged with rWIV1-SHC014S have experienced about 20% body weight loss by the 6th day post infection, while WIV1 and rWIV-4231S produced less body weight loss. In th emice infected with rWIV1 -WIV16S, no body weight loss was observed (Fig. 35a). 2 and 4 days post infection, the viral load in lung tissues of mice challenged with rWIV1-SHC014S, rWIV1-WIV16S and rWIV1-Rs4231 S reached more than 106 genome copies/g and were significantly higher than that in rWIV1-infected mice (Fig. 35b). These results demonstrate varying pathogenicity of SARSr-CoVs with different spike proteins in humanized mice.
In the year 2020, it appears that the contract was revised and extended for an additional FIVE years!
For this period (2020-2025, it appears that AIM 3 on the cover page was re-written to remove any gain-of-function research from the proposal front page. It is as if they might think that they could be blamed for having conducted gain of function research that resulted in development of a virus that was released onto the global population! Seriously, the complete rewrite of AIM 3 on the new contract cover page to remove all allusions to the creation of mutant viruses has the appearances of a cover-up of one of the most highly lethal atrocities in the world.
Aim 3. In vitro and in vivo characterization of SARSr-CoV spillover risk, coupled with spatial and phylogenetic analyses to identify the regions and viruses of public health concern. We will use S protein sequence data, infectious clone technology, in vitro and in vivo infection experiments and analysis of receptor binding to test the hypothesis that % divergence thresholds in S protein sequences predict spillover potential. We will combine these data with bat host distribution, viral diversity and phylogeny, human survey of risk behaviors and illness, and serology to identify SARSr-CoV spillover risk hotspots across southern China. Together these data and analyses will be critical for the future development of public health interventions and enhanced surveillance to prevent the re-emergence of SARS or the emergence of a novel SARSr-CoV.
It is interesting that deeper into the text, the proposal is a little more specific about AIM 3.
Aim 3: In vitro and in vivo characterization of SARSr-CoV spillover risk, coupled with spatial and phylogenetic analyses to identify the regions and viruses of public health concern. We will characterize the propensity of novel SARSr-CoVs to infect people in vitro using primary human airway epithelial cells and in vivo using the transgenic hACE2 mouse model. We will use mAb and vaccine treatments to test our hypothesis that SARSr-CoVs with 10-25% divergence inS protein sequences from SARS-CoV are likely able to infect human cells. and to evade mAb therapeutics and vaccines. We will then map the geographic distribution of their bat hosts and other ecological risk factors to identify the key ‘hotspots’ of risk for future spillover.
Note the use of the word “novel.” It is unclear if these novel mutants have already been “developed” (gain of function research) in prior years or whether they are to be developed.
Farther into the documents, they write (page 496):
3.3 Virus characterization: 3.3.a Construction of chimeric SARSr-CoV viruses: Infectious clones with the S gene of novel SARSr-CoVs and the SARSr-CoV WIV1 genome backbone using the reverse genetic system developed in our previous R01 (24). The correct infectious BAC clones will be screened by BAC DNA digestion with appropriate restriction enzyme or PCR amplification. The chimeric viruses will be rescued in Vero cells and then verified by sequence analyses.
The proposal goes on to describe how the chimeric viruses will infect primary epithelial cells and humanized mice (pages 496-497).
Yep! Nothing has changed. Deep in the text is the gain of function research that they still have left to do! It is just removed from the front page of the proposal.
The are no more annual reports – so whatever research has been conducted subsequently is not known past the 2019 annual report.
This research has to stop now. Congress must stop the funding immediately. There must be accountability. There must be justice for the injured and the dead.
There are ten million people dead from this research “project”. Do we need another man-made outbreak to fully grasp how dangerous this type of research is?
Just like Hunter Biden’s laptop was “misinformation” that turned out to be true. The “conspiracy theory” about the origin of Covid-19 has also proven true. –TPR
















![author['full_name']](https://i0.wp.com/clf1.medpagetoday.com/media/images/author/Putka_Resize_96.jpg?resize=50%2C50&ssl=1)