Visits: 27
Silent Lunch, The David Zweig Newsletter
Santa Clara County, California, imposed some of the harshest Covid restrictions in America. A church and its members defied them — and became the targets of an unprecedented surveillance operation


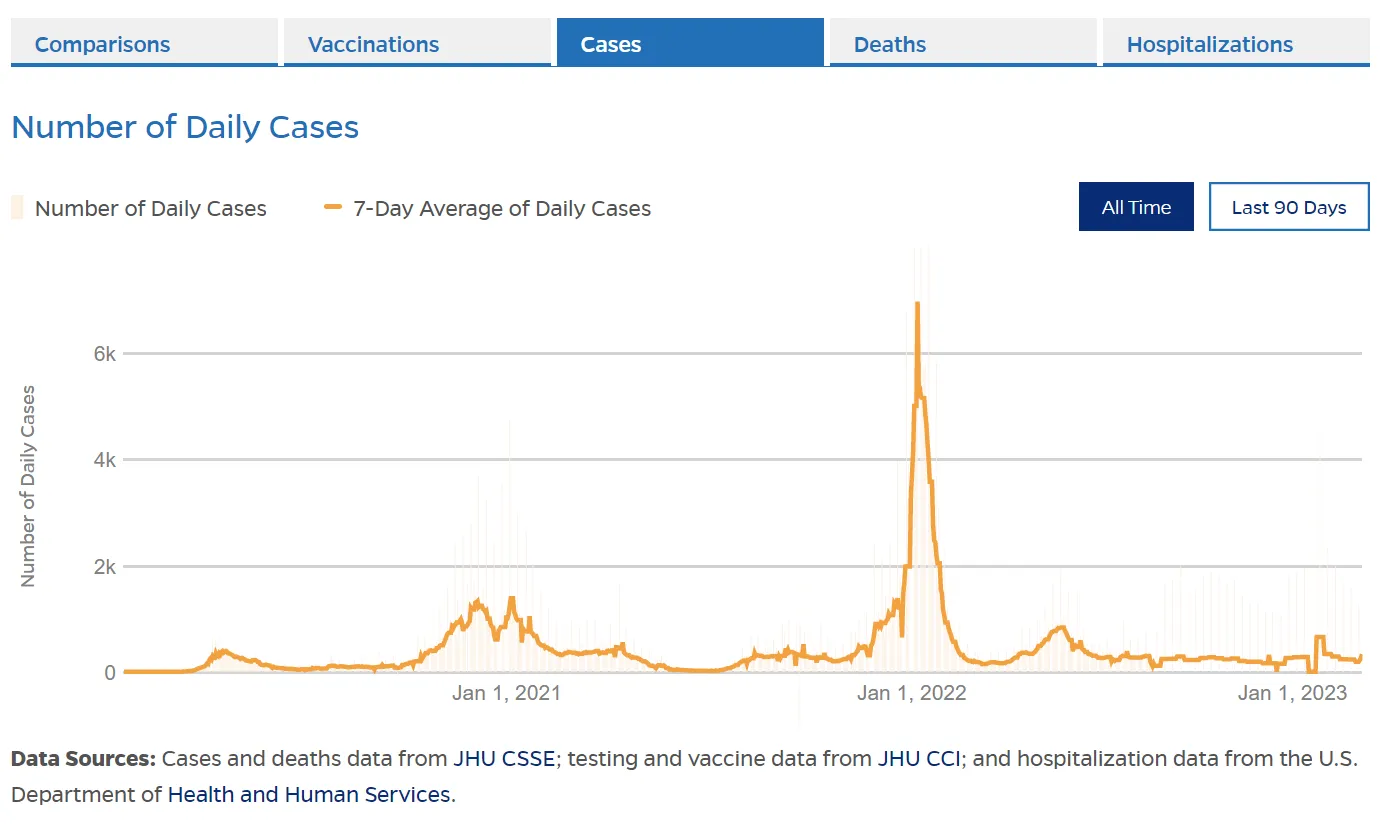
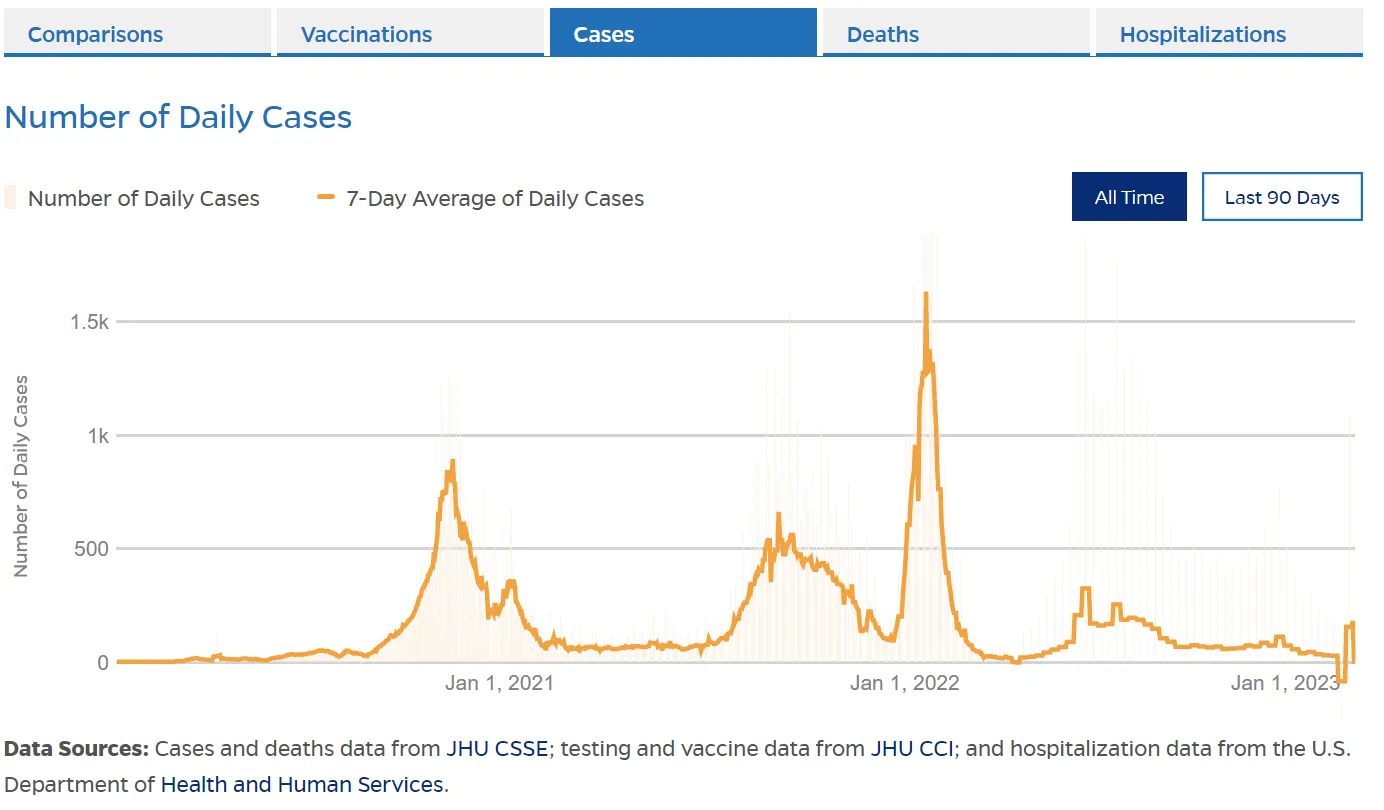
Long famous as the core of Silicon Valley, Santa Clara County, California, also earned the distinction in the last three years as perhaps the most aggressive and punitive enforcer of pandemic restrictions in the country. On March 16, 2020, Santa Clara, along with a half-dozen other Bay Area counties, was the first in the nation to announce a shelter in place order, commanding all citizens to remain at home other than for specific activities that the county deemed essential, such as food shopping or medical care. It wasn’t until mid-October — seven months after the initial order — that Sara Cody, the head of the county’s public health department, began allowing indoor gatherings at churches, provided they were no more than 100 people or 25 percent of a facility’s capacity, whichever was fewer. At these limited gatherings face coverings and social distancing were required, and singing was banned.
San Jose’s Calvary Chapel, led by its pastor, Mike McClure, brazenly defied these orders. On May 24, 2020, McClure stated publicly that he would reopen the church the following week, regardless of the health department’s orders, and that he would never close the church again. After two months of isolation, many congregants were teetering toward despair. They were suffering greatly from loneliness, depression, and crippling anxiety — the church was their community, and returning to the normalcy of its rituals and in-person fellowship was vital for their mental, spiritual, and physical well-being.
True to McClure’s word, at the end of May Calvary began holding indoor gatherings, often with hundreds of worshipers, a large portion of whom were without masks, in breach of distancing rules, and singing. This set off a collision between the openly defiant church and the county that culminated in two lawsuits. One, in federal court, in June 2020, by the church against the county, claiming the restrictions violated a list of constitutional rights, and the other, in state court, in October 2020, by the county against the church, for “flagrantly and repeatedly” violating public health orders and nonpayment of fines.
Both cases are still in litigation, but extensive legal documents, totaling more than a thousand pages, reveal a county, and its health department, that went to extraordinary, and potentially unlawful, lengths to enforce its decrees. These efforts include levying more than $2 million in fines against Calvary, and a multi-faceted surveillance program of the church and its members, breathtaking in scope and reminiscent of totalitarian regimes, rather than an American county health department — the spy operation included stakeouts, forced in-person monitoring of prayer groups and other intimate activities, and tracking the cellular mobility data of churchgoers.
The county’s public health orders, which were applied incongruently to different entities, and its enforcement mechanisms raise important legal and ethical issues about government infringements on citizens’ rights related to privacy, assembly, and religion that run well beyond the context of the pandemic and have potential implications for Americans regardless of their religious or political affiliation.
* * *
AN AGGRESSIVE COUNTY, AND ARBITRARY RULES
From the outset, Santa Clara had an unusual fervor for enforcing its health orders, and for punishing those who didn’t comply. By one analysis, as of March 2021, the county had issued an astonishing $4.9 million in fines to nearly 400 businesses and entities for pandemic rules infractions. By comparison, six other Bay Area counties combined had collected just $82,000.
Santa Clara’s aggressive stance can be traced back to August 11, 2020, when the county established a “civil enforcement program” for its public health orders. As part of the program, a Business Compliance Unit was created, composed of as many as ten or more enforcement officers, tasked with investigating potential violations of the health department’s orders. In public communications, the county asked residents to report on people and entities not in compliance with the health orders through a special hotline and website. To encourage citizens to rat out offenders, an explicit part of the enforcement system, detailed in the county’s Urgency Ordinance, was granting confidentiality to those who filed complaints.
On August 21, 2020, in response to one such complaint, Calvary was served with a cease-and-desist letter for holding indoor gatherings, for failing to ensure everyone wore masks, for failing to ensure social distancing, and for failure to ensure there was no singing. Two days later, enforcement officers arrived at the church and reported observing at least 100 unmasked people gathered inside, not distancing, and with some of them singing.
So began a series of issuances of fines for violations every single day, beginning in August, and running through the spring of 2021. The fines began at $1,000 each. Per the terms of the public health order, there was no grace period, and the amounts doubled each day that the violations were not corrected until a maximum of $5,000 per day was reached. By October 27, 2020, the county had already fined Calvary $350,000.
As I read the legal filings and reviewed the various public health decrees issued by Santa Clara authorities, something struck me as very odd. The church was accruing fines like John Bender racking up detentions in the Breakfast Club for breaching various orders; yet other aspects of society during that same time had very different restrictions.
In September, Santa Clara churches were still prohibited from any indoor gatherings, yet, by contrast, shopping malls could operate at fifty-percent capacity. By October 14, when county churches were then allowed the lesser of 100 people or twenty-five percent capacity, museums could run at fifty percent, and stores had no capacity limits placed on them at all.
Much of Santa Clara’s restrictions early on were tied to state requirements, which were harsher on churches than stores. But Santa Clara expanded the chasm between houses of worship and retail establishments beyond what the state prescribed. (Through multiple exchanges with a county communications officer, asking why malls had looser conditions than churches, I was not given an explanation.)
The seeming illogic and unfairness aside, the county was determined to steadfastly enforce its orders on Calvary and impose financial penalties with terms that would shame a loanshark. To achieve these goals the Compliance Unit sought to document — with exceeding care, and through multiple forms of surveillance — the infractions of the outlaw chapel.
* * *
STAKEOUTS, AND ON-SITE SURVEILLANCE
On August 23, enforcement officers from the county’s Business Compliance Unit began regular surveillance of the church. On the first visit they entered the premises, observed the congregants, and then left to write up a Notice of Violation for masking, gathering, singing, and distancing violations. When the officers returned shortly after to deliver the Notice they were denied entry and told to get off the property. From then forward, each Sunday the enforcement officers were locked out of Calvary. But this did not stop them.
Barred from the premises, the Unit struck an agreement with the law-abiding church next door to Calvary for the officers to set up camp there for their operations. Enforcement officers, often working in pairs, conducted dozens of stakeouts, spying on Calvary staff and members by peering at them through a chainlink fence from the adjacent property.
Among the hundreds of court documents filed in the state case are extensive declarations from multiple county enforcement officers. It is in these declarations where they describe in granular, mundane detail the illegal goings on at Calvary Chapel. Masking and distancing infractions of church greeters and of attendees being welcomed into the building were documented over and over again. The officers also surveyed the church’s several parking lots each week, counting the number of cars to estimate how many people were inside.

Note was even made of traffic directors, who obviously were working outdoors, for not wearing masks. And hugging — presumably a distancing violation — was also documented.

This scenario played out every week, each instance described with the same particulars in a Groundhog Day type cycle. Yet all this meticulous documentation seems strangely superfluous since Calvary recorded its services and made them available online, providing all the evidence the enforcement officers needed.

Every Sunday, for months, the officers went through the same drill. The chainlink fence, the tallying of cars, the watching the livestream of maskless churchgoers singing, congregating. It is hard to believe this was an actual law enforcement operation that went on for months on end. The sheer absurdity of it all — the hyper specificity, the repetition, the mundanity. Instead of envelopes of cash being handed off and tucked into suit jacket pockets or shots taken with a telephoto lens of steel briefcases containing contraband, the reports consisted of people hugging or not wearing a mask while directing traffic in a parking lot. The declarations recounting the surveillance read like stakeout scenes from a screenplay of a police comedy — earnestness played as farce, with the officers as the classic straight man.
Things took a turn in November, when a judge issued a temporary restraining order, which empowered the enforcement officers to enter the property, which they did on numerous occasions purposefully timed with scheduled church events.
It is here where the details of the declarations take on a more creepy quality. Often intimate activities, with people sometimes at their most vulnerable — mothers in small prayer groups; children in daycare — were subject to observation. Officers described being escorted to an event called Manna for Moms.

The officers said they did not want to disturb the gathering, and favored observing through a window. But they were there, surveilling a private event: 17 women, one infant, and two children were in the room where the gathering was held. Most maintained six feet of distance, but some were not wearing masks, and one person was singing.

Pastor McClure offered the officers a tape measure, but this was declined. (He also tried to gift them his wife’s book at one point, which was also “politely declined.”) Officers noted that “a gentleman who identified himself as ‘Chris’ recorded us with his mobile phone. Chris also was not wearing a face covering.”
The officers returned repeatedly, often specifically on days and at times they knew there would be gatherings, such as bible study classes, youth events, and on Sundays for services. The cataloging of church members, their actions, and violations continues in the declarations ad infinitum. Women drinking coffee in a hallway. In the church cafe 11 young adults gathered, not wearing masks or distancing. Another youth gathering was noted for having chairs “arranged in a manner that did not allow for social distancing.” The officers observed baptisms, describing McClure touching the faces of baptismal candidates and pinching their noses as he submerged them in water (presumably this was marked down as a double violation of not masking and not distancing).
I am generally unacquainted with court declarations, and found much of the tone and content to be of such awkward literalness about such pedestrian circumstances, that it achieved a sort of high art of dry humor. And yet, these were often personal, intimate moments that were being monitored by force. I ultimately found myself increasingly uncomfortable reading the declarations, thinking about government officers intruding, over and over, on these private ceremonies and gatherings.
* * *
THE MEMBERS
Anthony, a 29-year-old county social worker, was one of the many people being observed at Calvary. [Some names have been changed to protect members’ identities.] Why was he there, knowing that it was against the rules?
“I was having some really dark moments,” he told me. Around the time the pandemic started he had gone through a breakup, which devastated him. And then the restrictions kicked in and his depression began to spiral downward. Thoughts of suicide entered his mind.
The pandemic in the spring was “a scary time for everyone,” he said. “We were getting swamped with cases in May and June. People were hurting.” While he tried to help others, he desperately needed help himself. “It was hard for me to regulate my emotions,” he said. Going to church, an activity that had centered him for his whole life, spending time with the other congregants, conversing face to face with the pastors, was the one thing he had to keep himself from doing something truly awful. “Those two hours I spent there were the best two hours of the week. It brought comfort. Despite everything that was going on.”
While he recognized that Covid presented risks to himself and society, he didn’t understand why people could go to a liquor store but not church. He tested himself every other day, used hand sanitizer, and, at least initially, wore a mask. In part because most everything was closed, he generally kept his distance from people. He didn’t see how he was endangering anyone. And everyone at church chose to be there. As a healthy young man Covid posed a real but extremely small risk to him, he said. Whereas without the church he was in serious trouble.
In the spring of 2020, Bryan Wells, aged 37, lost his job selling motorcycles up in Marin County, where he lived, because the dealership closed when the economy shut down. “I was in a big motorcycle community, but even that ended,” he said. “No one wanted to go anywhere. My sister and brother in law didn’t want to meet in person.” Wells struggles with addiction and relies on his faith to keep himself from swaying. “Christ turns off the taste for the things you want to do but that are bad for you,” he said.
Wells got a new job at a dealership in San Jose (businesses related to transportation were allowed to stay open), and began commuting close to two hours each way before eventually moving to San Jose. Several customers told him about this church that was open, and he began to attend. For him, more than the isolation that the new norms created, was that everyone around seemed to be living in constant fear. For Wells, fear is toxic. Going to Calvary, being with people unafraid, gave him the strength he needed to stay off drugs and alcohol.
For Katie Truman, going to Calvary didn’t save her, but she believes without it her son, Jonathan, 21 at the time, would be dead. When the restrictions hit he lost his job as a plumber’s apprentice. He had an alcohol problem before this happened, but after “his drinking got so bad, we worried for his life,” she said. Katie and her husband didn’t know what to do or how to help him. They were alone, at home, and weren’t talking with anyone, and didn’t know how to find resources.
I asked her why she couldn’t have just called the pastor for advice. She seemed surprised at or confused by my question. The topic wasn’t something she and her husband could even conjure up to discuss. It was only after being in the church, in person, having fellowship, that she shared with others what was happening with her son. “When you have no hope for your child who you love so much, to know where to go for that hope when almost everything is shut down, it was . . .” she drifted off.
One of the pastors then told Katie about a program for her son. She gave Jonathan an ultimatum and he agreed to go. She believes the program saved his life. He stayed in it for a year, and is now living in the Northeast and got married.
* * *
TRACKING MOBILITY DATA OF CHURCHGOERS
For their work monitoring and documenting the crimes of Katie and her husband, Bryan Wells, Anthony, and hundreds of others, each enforcement officer was paid $219 per hour. Between November 25, 2020 and January 3, 2021, alone, there were 51 hours of on-site surveillance.
But the county did not stop there. As if the outside surveillance from the stakeouts, the on-site visits, and the freely available video evidence of services wasn’t enough, the county also had another, far more sophisticated tool at its disposal.
The Santa Clara County health department used cellular mobility data to track how many people were attending Calvary Chapel on any given day. I found this information in a remarkable declaration amid the legal documents, from a professor at Stanford Law School named Daniel Ho. A research team, led by Ho, was hired to analyze the data for Santa Clara county health officers.
Ho, who has an expertise in statistical inference and quantitative data analysis on public health, explained in his declaration how the process worked. The county paid to acquire the data from a firm called SafeGraph, a company that “aggregates information from 47 million mobile devices across the United States.” SafeGraph aggregates these data on points of interest (POIs), including daily visit counts.
A geofence — a virtual geographic boundary — was set up around Calvary Chapel’s property.

SafeGraph matches Global Positioning System (GPS) data to individual POIs by using “geographic shapefiles” — the red boundary runs the perimeter “shape” of the Calvary property, and the yellow boundaries indicate individual building shapes within the property. The data was so granular that Ho’s team differentiated daily visits to both the overall parcel of land, and to specific structures within the Calvary building complex. Once a device was in the geofenced area for four minutes it was counted as a visit.
Of the 47 million devices tracked by SafeGraph, approximately 65,000 during the study period were in Santa Clara County. Since this only represents a portion of all mobile devices, Ho’s team used statistical modeling to extrapolate the actual number of people coming to Calvary. Ho estimated that before the pandemic Calvary maxed out at 670 people visiting in one day. In early 2021 that number had exploded to a 1,700 person daily peak.
Should the lawsuit ever get to trial, the county plans to use Ho’s analysis of the SafeGraph data to show that Calvary was an outlier among POIs in general, and specifically among religious organizations, for daily visits. But it’s hard to imagine how this information bolsters their case beyond what was already known from the declarations recounting what was observed on the innumerable stakeouts and on-site visits. Moreover, the church has never disputed that it held services and other events. On the contrary, it has been overtly public about it.
The SafeGraph data ostensibly does not provide personal information on individuals. Yet I spoke with a scientist who utilizes similar data in their work who said it would, of course, be easy to identify an individual user. You can track the location at one POI, in this case the church, and then follow the device back to its home address. This isn’t to suggest that Ho or Santa Clara did this or had access to the movement data. But the point is an entity could easily figure out individuals’ identities if SafeGraph gave them the data.
Santa Clara was using SafeGraph data as early as November 2020 for general purposes as part of its pandemic initiatives. According to a member of the County Board of Supervisors, the Health Department wanted to track people coming in and out of the county to try to predict the impact of Thanksgiving. In a December 2020 meeting, where the data were reviewed, the member expressed concern about the data showing many Santa Clara residents traveling for the holiday to Southern California, where Covid rates were higher than in the Bay Area.
(It is not clear to me what was actionable about learning this, since the review was after the fact. And one can only conjecture about what the authorities could do with this information. Presumably the Health Department, under Cody’s direction, for example, was not considering an attempt at closing the County’s borders. Perhaps if they saw too many residents going somewhere they felt was dangerous, like LA, and then returning to the county, they would consider imposing harsher lockdown measures.)
Unsurprisingly, the top six POIs on the day after Thanksgiving were shopping centers and malls. It is worth noting that during that time churches were barred from any indoor gatherings.
For any readers who may think all of this data tracking is fine, especially so of the churchgoers, since they were breaking the law, you may want to take a breath here. Because surveillance is never limited to the people you disagree with.
According to a Vice exposé, SafeGraph also sold mobility data of people visiting abortion clinics, including more than 600 Planned Parenthood locations. The data showed “where groups of people visiting the locations came from, how long they stayed there, and where they then went afterwards.”
The CDC, along with a number of municipalities and researchers also track mobility data for epidemiological and other purposes. How these data are being used in every instance is unknown. The Santa Clara lawsuit, however, gives a rare window into a particularly egregious example of an American municipal government monitoring the whereabouts of its own people without their knowledge.
* * *
TO WHAT END?
Daniel Ho’s analysis of the SafeGraph data — for which the county paid him $800 per hour — appears to be correct. When I spoke with Pastor Mike McClure he confirmed that Calvary’s attendance exploded during the pandemic, roughly matching the numbers from Ho’s report. At a certain point Calvary began holding two Sunday services, with close to a thousand attendees in each. McClure also said that prior to 2020, he performed fifty to 100 baptisms a year. During the pandemic, and continuing now, he has averaged 1,000 each year. The church wasn’t just attended by its own members, but also by hundreds of people, like Bryan Wells, who weren’t members but came because it was the only spiritual place open.
The Calvary attendees I spoke with were not firebrands and provocateurs. They were not demanding on March 17, 2020 that barbershops be allowed to give haircuts. McClure told me the church membership runs the gamut from blue collar workers, to doctors and lawyers, construction contractors, and grocery store cashiers. These are everyday people who, after months of being denied what they felt they needed to thrive — and for some, to survive — were pushed to act, even though it was against the rules decreed by a county official.
None of the people I interviewed thought Covid was a hoax, or that the vaccine was a conspiracy by Bill Gates, or any other nonsense that has so often been ascribed to anyone who didn’t want to follow every Covid rule without questions. They just had a different risk benefit calculation than those made by the authorities, and after some time they felt backed into a corner to the point where they could no longer comply.
“We are law-abiding people,” Katie Truman told me. “And it was hard to think that people would think we didn’t care about them and that we were being defiant and disrespectful of them.” She said she couldn’t understand how banning the indoor gathering at the church made sense when casinos were open.
Each of the congregants I spoke with mentioned that while they were not dismissive of the harms of Covid, they were in church week after week, with hundreds, or more than a thousand other people, and there was nothing noticeable happening. In Calvary’s declarations they point out that there is no evidence that church attendees had a higher rate of Covid infections than the community at large.
In 2006, D.A. Henderson, a doctor who led the program to eradicate smallpox, and who was considered, before his death in 2016, perhaps the world’s most celebrated epidemiologist, wrote the following: “Experience has shown that communities faced with epidemics or other adverse events respond best and with the least anxiety when the normal social functioning of the community is least disrupted.”
Ironically, the SafeGraph data confirms the failure of Santa Clara’s public health orders. Government-imposed interventions only work to the extent that people are willing to follow them. One must question whether official rules are effective or reasonable when they compel a large number of good people to become criminals. The authorities said it would be two weeks, and didn’t adequately check in with the public to ask, “Hey, is it cool if we continue with this?”
In February 2021, the US Supreme Court struck down California’s ban on gathering in churches. As a result, Santa Clara has dropped its complaint against Calvary for gathering violations, and instead is only suing for masking violations. As is well-accepted now by nearly all public health officials, there is no evidence that cloth masks — the only kind that were mandated — have any meaningful benefit at the population level. Currently, the county is seeking $2.78 million, and a decision is expected this spring.
* * *
Producing an investigative feature of this depth and complexity requires extensive research, cultivating sources, interviews, writing, editing, and fact checking. I made this piece free for anyone to read because I believe it’s important for it to reach the widest audience possible. You’re not going to find this reporting in legacy media outlets.
![]()
 152
152